Watch the latest episodes of the Innovation Journal Club series on Eyetube.

The Innovation Journal Club series on Eyetube takes an in-depth look at podium data, peer-reviewed literature, and experiences from outside the United States related to innovations and technologies that offer to change the way ophthalmology is practiced in the real world. Hosted by I. Paul Singh, MD, of the Eye Centers of Racine & Kenosha in Wisconsin, the series is editorially independent, thus giving viewers an unvarnished and unbiased look at emerging trends in eye care. Each episode features interviews with leading experts from across subspecialities, which simultaneously broadens the scope of topics while also serving to sharpen the focus of the content of each discussion.
The following is a summary of three episodes in which Dr. Singh sat down with Sahar Bedrood, MD, PhD, a cataract and glaucoma surgeon in Los Angeles, to talk about innovations in glaucoma; with Mark Lobanoff, MD, of Ovo Vision in Minnesota, to explore developments in refractive surgery; and with Ralph Chu, MD, of Chu Vision in Bloomington, Minnesota, to discuss the advent of topical presbyopia treatment.
Innovations in Bleb-Forming Glaucoma Surgery
Featuring Sahar Bedrood, MD, PhD

While considered the gold standard for targeting robust IOP reduction, risks and complications associated with trabeculectomy warrant careful consideration and may disqualify some patients from the procedure. Newer surgical techniques and approaches may be a viable alternative in select cases, at least as an interim step before incisional techniques are needed. In episode 4 of Innovation Journal Club, host I. Paul Singh, MD, sat down with Sahar Bedrood, MD, PhD, to discuss two studies that compare minimally invasive bleb-forming procedures with trabeculectomy.
GPS: Gel Stent Versus Trabeculectomy
When it was introduced, the Xen gel stent (Allergan, an AbbVie company) ushered in a new category of glaucoma surgeries: minimally invasive, device-based, bleb-forming procedures. Whether they qualify as MIGS is not fully established, nor is the nomenclature to describe them. Nevertheless, due to a similar mechanism as trabeculectomy—facilitate nonphysiologic drainage to the subconjunctival space via a bleb formed postoperatively—they are intended to offer similar IOP-lowering efficacy, albeit with a more favorable safety profile.
According to Dr. Bedrood, the Gold Standard Pathway (GPS) Study was designed to help answer questions pertaining to patient selection and the clinical utility of the gel stent in eyes requiring modest IOP reduction. The safety and efficacy of the two procedures was compared in a head-to-head fashion in a 12-month, open-label, prospective, randomized, multicenter study. in 159 eyes (139 treated; 95 Xen, 44 trabeculectomy) with “poorly controlled glaucoma” (defined as IOP of 15–44 mm Hg on ≥1 topical medication).
The topline takeaway from the study was that gel stent was noninferior to trabeculectomy. Although trabeculectomy achieved slightly greater IOP lowering (Figure 1), the safety outcomes favored the gel stent (Table 1).
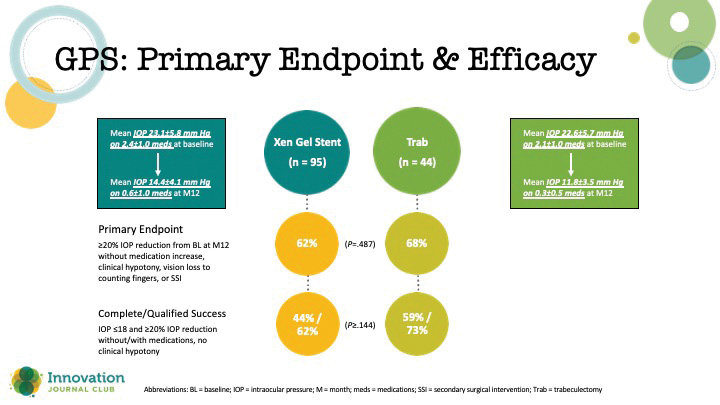
Figure 1. Primary endpoint outcomes in the GPS study.

Table 1. Safety outcomes in the GPS study.
“I love a good Trab,” Dr. Bedrood explained. “I always say that when I talk about Xen because there is a point where [a trabeculectomy] is important to do when you want those super low pressures, when you have a patient who is progressing at 13, 14 [mm Hg], and you want to try to get them down to 8 or 9 [mm Hg]. It may be worth the risk of this to get them down. But if you have a patient that doesn’t need that super low pressure, then let’s do the thing that has a higher safety profile at the end.”
According to Dr. Singh, the safety profile of the gel stent has made him more comfortable performing surgery earlier than he would have with a tube or trabeculectomy. Unlike trabeculectomy, which involves several surgical variables that effect the outcome (ie, flap thickness, size, and placement; sure placement, etc.), drainage is facilitated by a patent microstent, thus making IOP response more reliable.
“The post-op period [with the gel stent], for me, has been much more controlled and predictable,” Dr. Singh said.
Interim Analysis of Pivotal Study
Although the pivotal study for the PreserFlo Microshunt (Santen/Glaukos)—another miniature implantable stent that affects drainage to the subconjunctival space via a conjunctival bleb—did not meet its primary endopoint, it nevertheless demonstrated clinically meaningful efficacy in secondary endpoints and was associated with more favorable safety (Figure 2).1
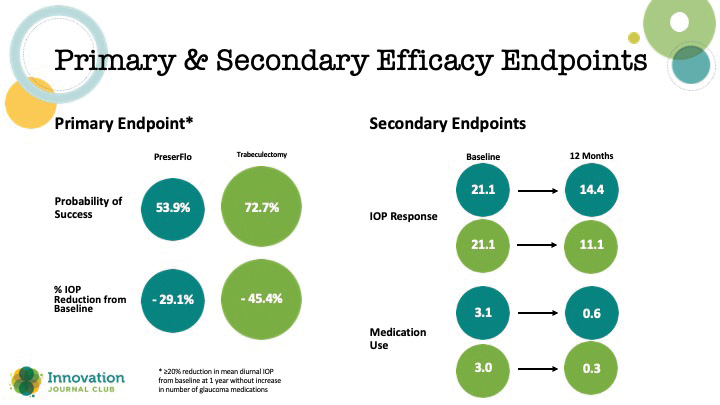
Figure 2. Primary and secondary endpoints in a study that compared PreserFlo to trabeculectomy.
According to Dr. Bedrood, the pivotal trial results should be viewed as only one piece of information about a promising device currently being reviewed by the FDA.
“I don’t see the fact that it didn’t meet that primary endpoint as being a game-over situation by any means. The standard was really high, and I think that there is definitely room to hopefully revisit this and reinvent it in a way that it’s applicable to our patients,” Dr. Bedrood said.
Dr. Singh added that interpreting outcomes from the study requires some context.
“It’s hard when you compare a new procedure to one that you’ve done for hundreds and hundreds of cases,” Dr. Singh said. “In this study, and the previous study we talked about earlier with GPS, trabeculectomies did better than historical data. So we’re getting better at trabeculectomy, it’s not that the, let’s say, PreserFlo didn’t work at all. In fact, it had significant reduction.”
What the blossoming category of minimally invasive, bleb-forming glaucoma surgeries ultimately offers, Dr. Bedrood said, is an answer to a current unmet need in clinical practice—the types of patients the ophthalmologist knows instinctually need a more aggressive approach to control IOP, but for whom the safety risks conjure a moment of pause. As well, she said, once a new device clears regulatory and enters the market, surgeons are likely to identify ideal patients, gain experience with the techniques, and thereby achieve better outcomes than witnessed in clinical trials.
1. Baker ND, Barnebey HS, Moster MR, et al; INN005 Study Group. Ab-externo microshunt versus trabeculectomy in primary open-angle glaucoma: one-year results from a 2-year randomized, multicenter study. Ophthalmology. 2021;128(12):1710-1721.
Innovations in Refractive Surgery
Featuring Mark Lobanoff, MD

New software rarely garners much attention. But when that software offers to improve surgical planning and result in more reliable and predictable postoperative refractive outcomes, it may be worth a deeper exploration to understand its impact for clinical practice. In episode 5 of Innovation Journal Club, I. Paul Singh, MD, interviewed Mark Lobanoff, MD, about two software development projects he is involved in.
Topography-Guided LASIK
According to Dr. Lobanoff, the release of topography-guided LASIK with Contoura (Alcon) was a game-changer in refractive surgery, conceptually offering the most accurate way to achieve a smooth, aspheric cornea. As he started to perform treatments, Dr. Lobanoff said he was generally pleased with outcomes but sensed there was room for improvement.
The fundamental issue Dr. Lobanoff identified with topography-guided LASIK is that treatment is planned based on the manifest refraction. Yet, each cornea has its own unique topographic pattern, with each peak and valley effectively creating a higher-order aberration (HOA) that affects the refraction of light. Manifest refraction considers the whole effect of HOAs but cannot discern the effects of each individual contour. In short, once any peak or valley is corrected, the manifest refraction theoretically changes as well.
“When you correct the topography, when you correct these hills and valleys on the cornea, the cornea that was in the phoropter that gave you that manifest refraction, it doesn’t exist anymore. When you’ve taken this mountain and you’ve reduced it, it’s a different cornea than what produced your manifest refraction. We needed a different way to calculate these treatments,” Dr. Lobanoff said.
Dr. Lobanoff’s proposed solution is the Phorcides Analytical Engine (PAE), an analytical engine to assist with Contoura LASIK treatment planning. By adapting to the cornea measurement principles used in the topographic analysis of the earth, the PAE provides a way to determine the actual low-order treatment astigmatism magnitude and axis. Briefly, the Phorcides Analytic engine:
- Assigns a refractive vector value to each area of topographic irregularity (called a talus) to calculate “true” low-order anterior corneal astigmatism.
- Incorporates posterior corneal data from a Scheimpflug device to calculate total cornea low-order astigmatism.
- Subtracts anterior and posterior corneal astigmatism from total astigmatism to calculate internal ocular astigmatism.
Clinical and refractive outcomes with Phorcides were assessed in a prospective, single-arm, interventional study at 4 clinics in the United States.1 Outcomes included UCVA and BCVA at 3 months and a patient questionnaire to assess quality of vision. Monocular refractive outcomes at 3 months are shown in the Figure.
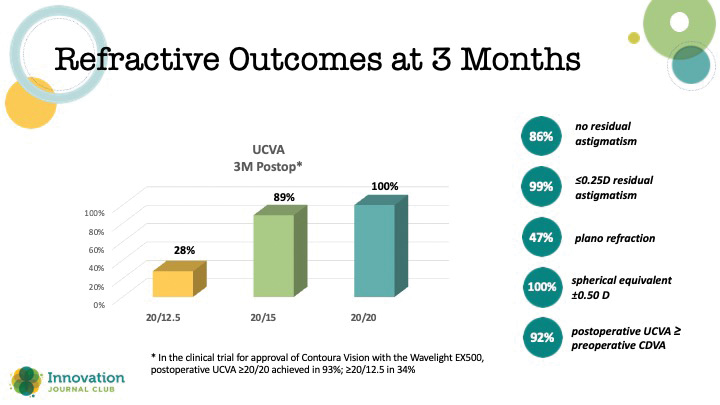
Figure. Refractive outcomes in a study assessing the Phorcides Analytical Engine.
For all of the complex mathematical computation that PAE performs, fundamentally, it brings in more data for analysis, including anterior and posterior corneal topography and manifest refraction, and then efficiently presents a treatment option for the surgeon to use or alter.
“It’s done the mathematics for you,” Dr. Lobanoff explained. “It’s done a lot of very complex computational features to it. But at the end of the day, the surgeon has to say, ‘I believe in this.’ They may modify it a little bit. And then they take that final treatment and put in the laser.”
Streamlined Refractive Cataract Surgical Planning
Another surgical software developmental program Dr. Lobanoff is involved with, eyeTELLIGENCE, a refractive cataract surgery planning platform, follows a conceptually similar algorithm as PAE: use more data to produce an improved treatment plan.
At a functional level, eyeTELLIGENCE (being developed in partnership with Baush + Lomb) pulls together data from various diagnostic devices (in a manufacturer-agnostic fashion), as well as pre- and postoperative information from the electronic records. The software also combs through a database built with artificial intelligence software to assess the most accurate IOL power calculation formula to use based on predefined anatomic or clinical characteristics.
“What does an IOL formula do? It gives you mathematical recommendations for this power lens should give you the best result. What we’ve been missing in ophthalmology is software that will tell you here’s the right formula to use,” Dr. Lobanoff said.
According to Dr. Lobanoff, if eyeTELLIGENCE works as expected, it is poised to reduce power calculation errors and thus help further refine postoperative outcomes. Yet it is also a platform upon which additional features can be integrated to reduce the potential for medical errors and provide the surgeon feedback on completed cases.
“What’s nice about eyeTELLIGENCE too is it also looks at your parameters as well. What’s going to be nice to see is when we start to look back at our data, If we change something in our technique, does that impact our efficiency and outcomes? And you’re going to have ways to look at that too, with eyeTELLIGENCE,” Dr. Singh said.
1. Stulting RD, Lobanoff M, Mann PM 2nd, et al. Clinical and refractive outcomes after topography-guided refractive surgery planned using Phorcides Surgery Planning Software. J Cataract Refract Surg. Published online Feb 10, 2022.
Innovations in Presbyopia Management
Featuring Ralph Chu, MD

The availability of pharmacologic management strategies for presbyopia has helped fill a treatment gap for patients who demonstrate the early signs of presbyopia. In episode 6 of Innovation Journal Club, Ralph Chu, MD, explains how this shifting paradigm represents an opportunity to advance the refractive mindset.
Topical Pilocarpine Phase 3 Study
The first entrant to the topical treatment category, pilocarpine HCl ophthalmic solution, 1.25% (Vuity; Allergan/AbbVie), mechanistically induces miosis. While pilocarpine is associated with the potential for adverse effects in high doses, Vuity is formulated in a low-dose formulation with a unique delivery vehicle that leaves the molecule inactive until it is introduced to the ocular surface—thus potentially reducing bioavailability to nontarget tissue.
Pilocarpine is a cholinergic muscarinic receptor agonist that acts through the M3 muscarinic receptor on the iris sphincter to constrict the pupil, thereby improving depth of focus via a pinhole effect. Reducing the pupil size to about 40% to 50% of its original dimensions provides an optimal range of focus that improves near vision without sacrificing distance.
In the phase 3 GEMINI study, Vuity demonstrated improvement in near vision without sacrificing distance under various lighting conditions.1 Furthermore, under mesopic conditions, the duration of effect was statistically significant out to 6 hours, and for intermediate vision, it was statistically significant out to 10 hours (Figure 1).
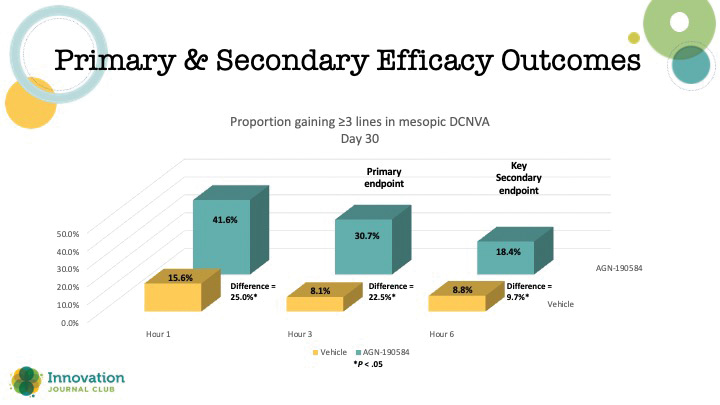
Figure 1. Primary and secondary efficacy outcome in the GEMINI 1 study.
“There is a secondary effect,” Dr. Chu said. “There’s a stimulation of the ciliary body. The cholinergic system causes sphincter contraction for the pupil, but it also causes accommodative spasm. And that’s important for our viewers because in some of those younger presbyopes who still have accommodative ability, like 40-year-olds, 41-year-olds, they might get a little bit of a myopic shift with this.”
There was a higher rate of headache, blurred vision, and redness in the active treatment arm compared to the vehicle, but overall, the drug was well-tolerated, and there were no serious adverse events. According to Dr. Chu, explaining the risks and benefits, as well as educating recipients on the potential to eliminate wearing glasses, might take on different prominence with this category of treatment. Because the treatment of presbyopia is not medically urgent per se, patients willing to try topical therapy may have different goals relative to those who are being treated with topical therapy for other ocular disorders.
“It’s really taking that mindset that this is not just a medical condition like glaucoma, where the patients have to take a medicine. We take a lifestyle approach. It’s really more about learning about what [the patient’s] needs are, and then I tell them about the limitations,” Dr. Chu said.
Presbyopia Classification System by Severity
The expanding array of presbyopia treatment options suggests an opportunity to customize a plan for each patient. One step in that direction, Dr. Chu said, is a recent publication proposing a new classification system by presbyopia severity.2
The expert panel focused on five clinical or patient features that help determine the degree of accommodative loss as well as how significantly it is affecting a patient’s near vision and lifestyle (Figure 2). Near add power was found to be the most significant indicator of presbyopic severity, while other factors (ie, behavioral/clinical findings, near visual acuity, and age) were found to be additive in refining classification of the presbyopia’s severity.
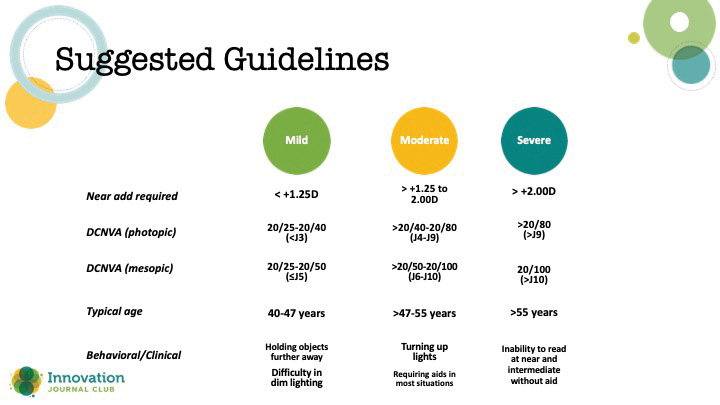
Figure 2. Suggested criteria for classifying presbyopia by severity.
“This study is one of the most important things that’s helped guide us in clinical practice,” Dr. Chu said. “Typically, in our conversations prior to this, it was just about age. ... But now that we’re looking more carefully at treating presbyopes, I’ve found that the Jaeger vision is the most effective counseling tool.”
1. Waring GO 4th, Price FW Jr, Wirta D, et al. Safety and efficacy of AGN-190584 in individuals with presbyopia: The GEMINI 1 Phase 3 Randomized Clinical Trial. JAMA Ophthalmol. 2022;140(4):363-371.
2. McDonald MB, Barnett M, Gaddie IB, et al. Classification of presbyopia by severity. Ophthalmol Ther. 2022;11(1):1-11.