
Editorially independent content, supported with advertising from New World Medical, Tarsus, and Trefoil Therapeutics
September 2023
I. Paul Singh, MD; Marguerite B. McDonald, MD, FACS; Charles C. Wykoff, MD, PhD; and Blake K. Williamson, MD, MPH, MS
In the Innovation Journal Club (IJC) series on Eyetube.net, host I. Paul Singh, MD, of The Eye Centers of Racine & Kenosha in Wisconsin, interviews leading experts from across eye care subspecialties about emerging innovations and technologies that may prove influential to the real-world practice of ophthalmology. The series is editorially independent (supported by advertising from multiple companies), which allows the discussions to be broad in scope and candid in presentation.
The following summarizes episodes in which Dr. Singh sat down with Marguerite B. McDonald, MD, FACS, to talk about the many potential applications for a drug that recently demonstrated the ability to treat night vision disturbances; with retina expert Charles C. Wykoff, MD, PhD, about the emerging treatment paradigm in geographic atrophy; and with Blake K. Williamson, MD, MPH, MS, about the growing use of MIGS among comprehensive ophthalmologists.
One example of a molecule with several potential applications is phentolamine ophthalmic solution 0.75% ([PMOS]; Nyxol; Ocuphire Pharma), an alpha-adrenergic agonist that modulates the pupil’s size by inhibiting the α1 receptors located on the iris dilator muscle.
A recently completed study, according to Marguerite B. McDonald, MD, FACS, is for treatment of visual distortions at night, which would benefit not only RK or LASIK patients complaining of unwanted photic phenomena, and patients with corneal scars, but also for patients with early anterior cortical cataracts who do not yet meet the criteria for cataract surgery. “There are a host of people in our offices who say, ‘I can drive at night if I have to, but I prefer not to.’”
Dr. McDonald joined Dr. Singh in an IJC episode to discuss the potential clinical uses of PMOS.
A phase 2 trial evaluated the use of PMOS for treatment of night vision disturbances.1 In the randomized, double-masked, placebo-controlled clinical trial, efficacy outcomes, including change from baseline in pupil diameter, contrast sensitivity, and VA, showed promising outcomes (Figure 1).In addition, patients in the PMOS arm also had greater mean change in pupil diameter from pre- to post-treatment (-1.3 mm [0 to -2.8 mm, P < .0001]) compared to placebo (−0.2 ± 0.5 mm, P = .08).
_1695732802.jpeg)
Figure 1. Mesopic low contrast VA in patients with known night vision disturbances in a phase 2 trial comparing 0.75% PMOS and placebo.
“And,” added Dr. McDonald, “not only did the effect not wear off, it got greater at 2 weeks. They actually got a little more effect at 2 weeks than they did the first time they tried it.”
Topline results from a phase 3 study, called LYNX-1, confirmed efficacy and safety demonstrated in the phase 2 effort, with 13% of PMOS compared to 3% in the placebo arm achieving the primary endpoint of ≥ 3-line improvement in low contrast distance VA.2 Dr. McDonald noted that adverse events in both studies were predominantly mild and did not lead to discontinuation of the drop.
Improving contrast sensitivity, especially at night, is something ophthalmologists readily understand to be beneficial. When Dr. Singh admitted to some difficulty in communicating this to patients, Dr. McDonald said she uses a dramatic example with her patients:
“I'll say, when we improve your contrast sensitivity when you're driving at night in the rain, you'll better be able to see that little girl in the gray raincoat as she steps off the curb.”
Although PMOS is not yet US FDA-approved, Dr. McDonald said there could be several potential uses for PMOS in ophthalmology, including presbyopia (the phase 2 portion of VEGA-1 is complete; the phase 3 VEGA-1, -2 study program has been initiated) and reversal of mydriasis for patients who are dilated during an eye exam who want quicker reversal of mydriasis.
Particularly notable, according to Dr. McDonald, is the long duration of action—18 hours in clinical trials—relative to some of the cholinergic agents available now or available soon for the treatment of presbyopia. Whether any difference translates to outcomes is yet to be understood, but that fact at least warrants further study, she said.
1. Pepose J, Brigell M, Lazar E, et al. A randomized phase 2 clinical trial of phentolamine mesylate eye drops in patients with severe night vision disturbances. BMC Ophthalmol. 2022;22(1):402.
2. Press Release. Ocuphire announces positive topline results from LYNX-1 phase 3 trial evaluating Nyxol® eye drops for night vision disturbances. May 19, 2022. Available at: https://ir.ocuphire.com/press-releases/detail/374/ocuphire-announces-positive-topline-results-from-lynx-1. Accessed July 27, 2023.
Ophthalmology marked a milestone on February 17, 2023, the day that the first complement inhibitor was approved for treatment of geographic atrophy (GA).
The approval of Syfovre (pegcetacoplan, Apellis) opens a new chapter as a first-in-class treatment. It was followed closely by avacincaptad pegol (Izervay, Iveric Bio), which gained the nod from the US FDA on August 5th, 2 weeks before its expected PDUFA date.
While it is too early to know what effect the introduction of complement therapy will have on GA moving forward, the approvals represent an important step ahead, according to retina expert Charles C. Wykoff, MD, PhD, who joined IJC for a virtual episode.
(Editor’s Note: This episode was filmed after the introduction of pegcetacoplan and before the approval of avacincaptad pegol).
“I believe GA has been one of the largest unmet needs in ophthalmology for the last 10 years, and we finally have a treatment for it. The treatment is a valuable, clinically meaningful step forward, but it has challenges, and we must continue to study them, learn from them, and eventually improve our therapeutics based on these learnings,” Dr. Wykoff said.
Some may be quick to compare this dawning era to the introduction of anti-VEGFs. However, with anti-VEGF therapy, response is often rapid, vision improves, and imaging changes over time. Those sorts of endpoints have not yet been established for GA.
“There were a lot of positive feedback loops with the anti-VEGF agents, with vision and anatomy both improving in most patients. It is a very different landscape with our current GA therapies which slow anatomic worsening but do not have a large, direct benefit on visual function within the time-frames or patient populations studied to date with these drugs,” Dr. Wykoff said.
According to Dr. Wykoff, “the complement system is part of the innate immune system that is important for protecting our tissues from infectious diseases and also important for clearing damaged tissues. What we think may be happening at a simplistic level … is that maybe macular degeneration is being driven at least in part by an overactive complement cascade in the back of the eye in these sensitive tissues, causing slow accumulation of cell death over a lifetime of the patient.”
Thus, therapeutic inhibition is rational. To date, clinical trials have shown benefit in inhibiting C3, which is the common convergence point of the three known activating pathways (ie, pegcetacoplan), or C5 (ie, avacincaptad pegol), downstream from C3, but prior to the terminal pathway involving formation of membrane attack complex, the primary driver of cell death, including death of the retinal pigment epithelium (RPE).
Overall, results from both treatments appear comparable, though have never been directly compared in studies. How they are interpreted may be crucial to understanding their utility. On the one hand, each is associated with only modest improvements in reduction of geographic atrophy (Figure 2). 1-3 On the other hand, from the patient perspective, the potential to preserve vision means things like greater independence and better quality of life.
_1695733100.jpeg)
Figure 2. Comparison of complement inhibitors that have reached phase 3 or later.
As with any pharmaceutical product, safety must be discussed. Each medication has a unique profile, but some commonalities exist, including potential intraocular inflammation, ischemic optic neuropathy, and development of wet age-related macular degeneration (AMD). The latter raises an important point about monitoring for all ophthalmologists to be aware of if they have a patient undergoing complement inhibiting therapy.
“A key is to obtain consistent OCT imaging in patients who are receiving treatment to evaluate for early signs of exudation, which could be an indication of development of wet AMD. There are extensive data showing that the earlier wet AMD is diagnosed and the sooner patients receive appropriate treatment, the more likely patients are to achieve optimal outcomes,” Dr. Wykoff said. “We don't want to miss an early conversion to wet AMD in these patients.”
Readers of the phase 3 clinical trials for complement therapies will note frequent reference to fundus autofluorescence imaging (FAF). Although it is invaluable for measuring GA progression, FAF is infrequently and inconsistently used by ophthalmologists, “even retina specialists,” Dr. Wykoff said.
GA is characterized by death of the RPE, which appears on FAF as dark spots, or a hypoautofluorescent signal. When that spot is rimmed by a bright hue, a hyperautofluorescent signal, it means the atrophy is at risk of expansion, as the adjacent RPE cells are unhealthy.
While assessing risk for GA progression is well characterized with FAF, OCT b-scans are still the most commonly employed tool for making a diagnosis and managing patients with GA (en face may be helpful for mapping progression over time). Among the hallmark signs, hypertransmission, or passage of signal through the choroid, may be one of the most distinctive.
“There's increased signal in the choroid from the OCT because there is less attenuation by the photoreceptors and the RPE. If you see a bright signal in the choroid, which you normally don't, normally the choroid is slightly dark and shadowy … that’s a signal that there may be overlying areas of atrophy,” Dr. Wykoff said, adding that other diagnostic clues exist including sharp linear lines interspersed with darkened areas (potentially referred to as a barcode sign).
1. Apellis. Press release, August 24, 2022.
2. Khanani AM, et al. Presented at: Retina Society; November 2-5, 2022.
3. Danzig C. Presented at: ARVO 2023; April 23-27, 2023. New Orleans, La.
Anyone with an interest in ophthalmology over the past decade or so has heard of MIGS. Its impact, though broad, is well understood. Despite that the category of minimally invasive surgeries has evolved and grown, the central premise remains true: achieve modest IOP reduction with a safe procedure associated with minimal postoperative recovery and rapid visual recovery.
One factor that may drive the next evolution in MIGS is that performing these surgeries is no longer the sole purview of subspeciality trained glaucoma surgeons, and that is in fact the best possible scenario for patients. At a fundamental level, more cataract and refractive surgeons performing MIGS, even in standalone settings, represents a wider pool of experience from which best-practices in clinical practices, and such things as patient selection, can be delineated.
Blake K. Williamson, MD, MPH, MS, joined an episode of IJC dedicated to taking a deeper look at this changing paradigm.
MIGS is associated with several positive outcomes. The library of studies demonstrating postoperative IOPs in the mid-teens in eyes with mild to moderate open-angle glaucoma is deep and convincing. Evidence of safety, pertaining to the class and to its members, is overwhelming.
Other endpoints, technically considered secondary in clinical studies, may be just as important. For instance, a few studies to date have pointed to the potential to forestall the necessity for incisional glaucoma procedures if MIGS is performed earlier in the disease course. There is also emerging evidence that some MIGS procedures are associated with greater preservation of visual field compared to drops.
From the patient perspective, the more-than-likely reduction in drop burden after a MIGS procedure may promote the health of the ocular surface. According to Dr. Williamson, drop burden reduction is even more meaningful when the impact on how that affects quality of life is considered.
“I think that what shocks me when I'm talking to my refractive buddies is that many patients are every bit as happy to get off medications as they are to get out of glasses,” Dr. Williamson said. “We always celebrate getting [patients] out of readers, getting [patients] out of contacts. But patients absolutely love being able to reduce their medication burden.”
MIGS is “the right thing to do for our patients,” Dr. Williamson added. But the real reason he incorporates MIGS in both combined and standalone settings into his surgical armamentarium?
“Happier patients,” he said.
The importance given to potential IOP reduction, and then magnitude of reduction after that, is in some respects understandable, given their utility for clinical trials, clinical practice, and for regulatory purposes. In MIGS surgeries in the real world, however, those endpoints may underrepresent the true impact. Indeed, achieving the target pressure after an uncomplicated MIGS procedure is a laudable endpoint, as is reduction of medications. But there is still more to the story of how success is defined, according to Dr. Williamson.
“Yes, that's a home run, but sometimes all you need is a single or double. I think that preventing further surgery, I think that's a success. Let's say that their pressure doesn't get any worse, and at least you're not having to add medications and you're preventing that incisional surgery for later. You're kicking the can down the road, saving some real estate. That's success too. While it's nice to present studies that show 30 to 35% IOP reductions and reductions in medication burden, I think it's also important to highlight that that's not the only way to create what we call success with MIGS surgery.”
Summing up his message to his fellow front of the eye surgeons, Dr. Williamson suggested to “consider the alternative, and the alternative is inertia, doing nothing, adding more drops, waiting for field loss, and boy, that doesn’t sound good if it were my family.”
Dr. Williamson reviewed data from two different MIGS devices that he said typify what he sees in real-world practice.
The first was a review of 12-month outcomes after the STREAMLINE Surgical System (New World Medical) in Hispanic patients with mild to moderate POAG. Dr. Williamson said that what he appreciated was that the baseline IOP of ~16 was indicative of the patients in his own practice (Figure 3).1 The second was a study in which Dr. Williamson served as lead author: 24-month data from the ROMEO study, an effort to understand longer-term outcomes with the OMNI Surgical System as a standalone procedure or combined with cataract surgery. Of note, the study reported IOP response stratified by baseline IOP: >18 mm Hg vs ≤18 mm Hg (Figure 4).2 Intergroup difference was less important than providing clinicians a framework for understanding outcomes in patient types representative of individuals who walk through clinic doors each and every day.
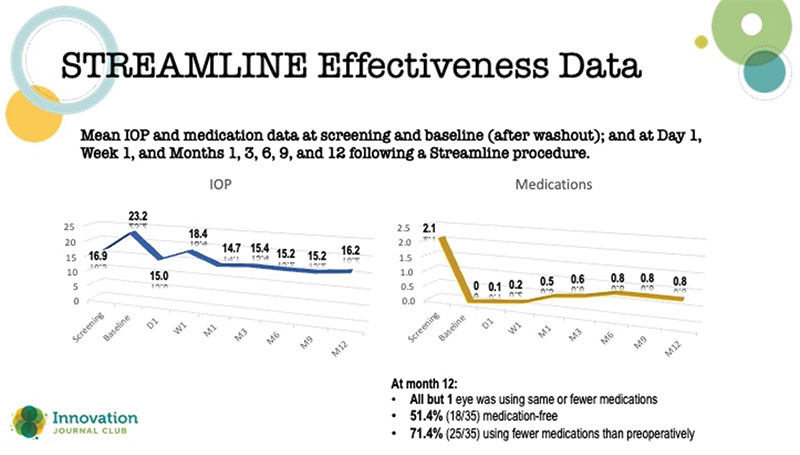
Figure 3. Results from a 12-month study of STREAMLINE.
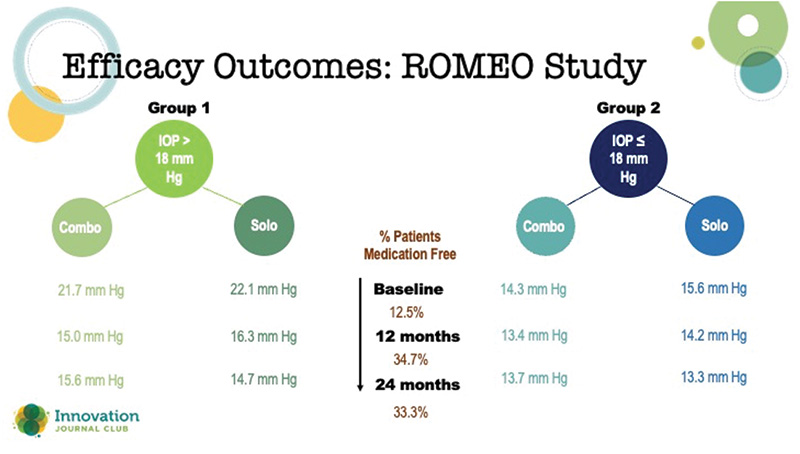
Figure 4. Two-year data from the ROMEO Study with the OMNI.
1. Lazcano-Gomez G, Antzoulatos GL, Kahook MY. Combined Phacoemulsification and STREAMLINE surgical system canal of schlemm transluminal dilation in eyes of Hispanic patients with mild to moderate glaucoma. Clin Ophthalmol. 2023;17:1911-1918.
2. Williamson BK, Vold SD, Campbell A, et al. Canaloplasty and trabeculotomy with the OMNI system in patients with open-angle glaucoma: two-year results from the ROMEO Study. Clin Ophthalmol. 2023;17:1057-1066.




