Sponsored by STAAR Surgical
May 2023
Expanding Surgical Options for Myopic Patients With EVO ICL Lens (EVO)
Alan R. Faulkner, MD; Deepinder K. Dhaliwal, MD, L.Ac; Sabrina Mukhtar, MD; Eva Kim, MD; George O. Waring IV, MD FACS; and Robert T. Lin, MD
The ICL is not just for patients who don’t qualify for LASIK.
More than 2 million EVO lenses have been distributed worldwide. Use of the procedure, which no longer requires a peripheral iridotomy thanks to a central port in the middle of the lens, is expanding. It is not just for patients who are not suitable for laser vision correction. Surgeons have reported excellent results for the treatment of as low as -3.00 D of myopia.1 EVO is becoming an excellent option for patients with low and moderate myopia.
Myopia is a global epidemic. In 2020, an estimated 34% of the global population was myopic, and it is expected to grow to 50% by 2050.2 Assuming the estimates are accurate, about 70 million people are currently living with myopia. Six million frequent replacement contact lens wearers drop out each year in the United States alone.3,4 The volume of patients searching for myopic surgical solutions therefore should continue to increase (Figure 1).

Figure 1. Statistics on the existing myopia market. Source: BHVI, adapted from Holden et al. 2016 Ophthalmology.
There is ample room for all refractive surgical technologies in your practice. Offering a variety of solutions, including EVO, can synergistically bring more patients into your clinics for refractive solutions. The following articles share advice from experts who have experience with EVO. They touch on patient selection, patient education, preoperative examinations, intraoperative pearls, patient outcomes, and growing your practice with EVO.
1. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:2981-3991.
2. Holden BA, Wilson DA, Jong M, et al. Myopia: a growing global problem with sight-threatening complications. Community Eye Health. 2015;28(90):35.
3. Nguyen TL. How to reduce contact lens dropouts. June 28, 2017. Accessed April 20, 2023. https://www.reviewob.com/4-steps-to-reduce-contact-lens-dropouts-increase-profitability/
4. Rumpakis J. New data on contact lens dropouts: an international perspective. January 15, 2010. Accessed April 20, 2023. https://www.reviewofoptometry.com/article/new-data-on-contact-lens-dropouts-an-international-perspective
Make a strong recommendation for appropriate candidates.
I have extensive experience with EVO ICL lenses (EVO). Talking to patients about the technology therefore comes naturally to me. Even so, the introduction of EVO has made my conversation with patients even easier because surgery is more streamlined now that a preoperative laser peripheral iridotomy is no longer required. Focus on five main points when educating patients on EVO:
We tell patients EVO works in harmony with their natural eye, similar to adding a lens to a camera, and explain that it is made from a collagen-containing safe and biocompatible material that also provides UV protection. We explain that EVO is soft, flexible, and invisible to them and others—making it feel like the lens isn’t even there apart from the fact that they are experiencing great vision.
Patients are educated on how the lens works. We describe that EVO functions similarly to their glasses or contact lenses to correct myopia and myopic astigmatism and that it creates sharp, clear vision by focusing light on the retina.4 We share that the technology has been used for more than 20 years and more than 2 million ICLs have been distributed worldwide.
According to one survey, 99.4% of patients reported they would have the EVO procedure again.2 Patients report exceptional vision throughout the day without compromising night vision.4,5 Additionally, we share with patients that EVO is clinically proven to not cause or contribute to dry eye syndrome.6
We share that EVO can be removed by a doctor, if necessary (although it is extremely rare), and does not involve removal of corneal tissue. This, we explain, ensures that they have maximum flexibility for IOL selection in the future when cataract surgery is required. On the other hand, post-LASIK patients might not qualify for premium IOLs and because making accurate IOL calculations in post–laser vision correction corneas can be challenging.
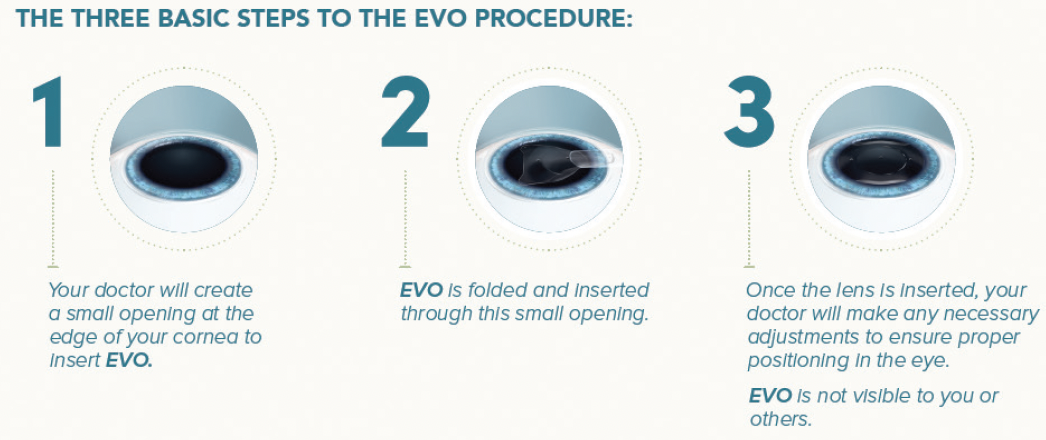
Patients like to hear that, in my hands, the EVO procedure is done in approximately 15 minutes and three easy steps (Figure 1). They are told that they will first receive eye drops to dilate and numb their eyes, and afterward, the surgeon creates a small opening at the edge of the cornea, implants EVO through the incision, and dials it into position behind the iris and in front of the natural lens to ensure proper positioning.

Figure 1. The three basic steps of the EVO procedure.
We talk a lot about the difference in invasiveness between EVO and laser vision correction because some patients perceive EVO as more invasive than LASIK since we actually go inside the eye during surgery. We talk to them about the amount of area that is disrupted in the cornea by making a flap as compared to EVO, where we make two very small incisions and remove no tissue. This conversation has really shifted the way patients look at the procedure.
A review of the moderate myopia results from the US FDA clinical trial of the EVO confirms that the lens is accurate, predictable, and stable for the correction of moderate myopia and myopic astigmatism and that it provides high levels of uncorrected distance visual acuity (UDVA).1
A retrospective review was conducted on a subset of patients from the US FDA clinical trial. Data for 200 eyes of 114 patients (mean age, 35.1 ±5.1 years; range, 21-45 years) with a preoperative manifest refraction spherical equivalent (MRSE) between -3.00 and -6.00 D (mean, -4.61 ±0..87 D) and astigmatism up to 4.00 D who completed at least 6 months of follow-up after EVO surgery were evaluated. All procedures during the multicenter trial were conducted under US FDA Investigational Device Exemption.
At the 6-month follow-up visit, the MRSE improved to -0.085 ±0.26 D. All patients were within ±1.00 D of the intended refraction, and 91.5% were within ±0.50 D. Also at 6 months, mean UDVA and corrected distance visual acuity (CDVA) were -0.065 ±0.08 and -0.14 ±0.07 logMAR, respectively, with most eyes (98%) maintaining or gaining lines of CDVA. No eye lost more than 1 line of CDVA.
Regarding efficacy and safety, the indices were 1.03 and 1.21, respectively. There was no incidence of pupillary block, anterior subcapsular cataract, or elevated IOP due to angle narrowing or pigment dispersion. The mean endothelial cell density decreased by 2.2%, and no eye required a pre- or postoperative peripheral iridotomy or iridectomy.
1. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
In the past, some surgeons reserved the ICL only for patients with high myopia and thin corneas. EVO, however, is appropriate for most patients with -3.00 D or more of myopia or myopic astigmatism. The US FDA clinical trial of EVO showed the lens provides excellent quality of vision including low and moderate myopia (see US FDA Clinical Trial: Review of Results for Moderate Myopia).7 In Hawaii, where I practice, about 70% of the population is of Asian descent. As a result, the rate of myopia is extremely high, and we don’t have to look hard to find patients who are good candidates for ICL surgery. With EVO, we have increased our pool of patients even further, allowing us to treat those who would have previously been turned away from surgery.
1. Schild G, Amon M, Abela-Formanek C, Schauersberger J, Bartl G, Kruger A. Uveal and capsular biocompatibility of a single-piece, sharp-edged hydrophilic acrylic intraocular lens with collagen (Collamer): 1-year results. J Cataract Refract Surg. 2004;30(6):1254-1258.
2. Brown DC, Ziemba SL. Collamer intraocular lens: clinical results from the US FDA core study. J Cataract Refract Surg. 2001;27(6):833-840.
3. Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. 2018;12:2427-2438.
4. Martínez-Plaza E, López-Miguel A, López-De La Rosa A, et al. Effect of the EVO+ Visian Phakic Implantable Collamer Lens on visual performance and quality of vision and life. Am J Ophthalmol. 2021;226:117-125.
5. Parkhurst GD. A prospective comparison of phakic collamer lenses and wavefront-optimized laser-assisted in situ keratomileusis for correction of myopia. Clin Ophthalmol. 2016;10:1209-1215.
6. Ganesh S, Brar S, Pawar A. Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism. Clin Ophthalmol. 2017;11:1253-1263.
7. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
Reliable data is key.
The EVO ICL lens (EVO) opens refractive surgery up to a huge patient population. In addition to two full-thickness peri-optic ports and two full-thickness ports on the footplates, EVO has a novel 0.36-mm central port (Figure 1) that effectively allows physiologic aqueous flow. This results in an exceedingly low risk of pupillary block and anterior subcapsular cataract and eliminates the requirement for a preoperative peripheral iridotomy.1 Because aqueous can flow through the anterior segment and nourish the crystalline lens, IOP is well controlled while maintaining the quality of vision patients experience with this lens. Long-term evidence has shown that visual quality is excellent in eyes with moderate to high myopia.2 Now, current evidence also shows that EVO is an effective treatment for as low as -3.00 D of myopia.3

Figure 1. EVO uses advanced technology to provide outstanding safety.
Our experience has taught us that, regardless of the amount of refractive error, nailing the preoperative examination is the first step in achieving excellent outcomes with EVO.
Following a precise and straightforward preoperative evaluation process will help eliminate the outliers and enhance surgeon confidence in the EVO procedure. The preoperative exam for EVO is like any refractive surgical evaluation. The ocular surface, crystalline lens, iris, and retina are assessed. For EVO, the anterior chamber depth (ACD) is then measured with a device such as the Pentacam (Oculus). EVO is indicated for an ACD (true ACD) of 3.0 mm or greater. Additionally, we like to use ultrasound biomicroscopy (UBM) to look for iris or ciliary body cysts and anterior segment OCT to assess sulcus-to-sulcus measurement.
EVO sizing affects the vault, which should be approximately 250 to 900 µm.4 The standard method for ICL sizing is to obtain white-to-white measurements and import them into STAAR’s online calculator and ordering system (https://ocos.staar.com/). Another alternative is sulcus-to-sulcus measurements.
We use several devices to help with sizing, including the IOLMaster (Carl Zeiss Meditec), Lenstar (Haag-Streit), and Visante (Carl Zeiss Meditec). Note that it is not an FDA requirement to obtain multiple measurements. The basic requirement for sizing, according to the US FDA, is white-to-white diameter. All you need to feel comfortable picking a size for EVO is a single reliable way to look at white-to-white (or sulcus-to-sulcus) and anterior chamber depth. Having other diagnostic equipment available is helpful but by no means necessary.
The surgical skill set required for cataract surgery converts into EVO surgery easily—much easier than phacoemulsification to LASIK. If you’re a careful, delicate cataract surgeon and can do a smooth procedure, then you can be an awesome ICL surgeon after completing the EVO certification training. For beginning surgeons, visit a surgeon who has a meticulous surgical technique with EVO or watch a surgical video of somebody who has a simple and predictable technique from start to finish. Our cornea/refractive surgery fellows at the University of Pittsburgh are certified to perform EVO surgery, and their results starting with their first case are the same as more experienced surgeons since they adopt the same technique. Our four top tips are the following.
In reality—with EVO—the vault is very forgiving. This doesn’t mean we shouldn’t measure the vault or pay attention to it, but selecting a lower vault, when appropriate, should not be concerning. The occurrence of cataract with the current model is rare. There were no cases (0.0%) of anterior subcapsular cataract in the US FDA clinical trial for EVO at 6 months and none reported in a review of the worldwide literature covering 4,196 eyes implanted with EVO lenses.3,5
Preoperative measurements are important for sizing EVO properly. With practice and the right strategy (for more surgical tips, see the sidebar above), it becomes easier to nail the intended outcome and provide patients with the best opportunity for superb vision after surgery.
1. Packer M. Evaluation of the EVO/EVO+ Sphere and Toric Visian ICL: Six month results from the United States Food and Drug Administration clinical trial. Clinical Ophthalmology. 2022;16:1541-1553.
2. Niu L, Miao H, Tian H, Ding L, Wang X, Zhou X. Visual outcomes of Visian ICL implantation for high myopia in patients with shallow anterior chamber depth. BMC Ophthalmol. 2019;19:121.
3. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
4. Alfonso JF, Fernandez-Vega L, Lisa C, et al. Central vault after phakic intraocular lens implantation: Correlation with anterior chamber depth, white-to-white distance, spherical equivalent, and patient age. J Cataract Refract Surg. 2012;38:46-53.
5. Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. 2018;12:2427-2438.
The procedure is simple and quick, and the lens is removable by a doctor if needed.
It’s incredibly rewarding to have a patient tell you after surgery that the vision you gave them is the best vision they’ve ever had. In my experience, this reaction istypical of EVO ICL lens (EVO) patients. I’m used tohearing them express that their vision after surgery exceeds theirexpectations. Now that EVO is approved in the United States and surgery is a moreefficient process, their overallexperience is better as well. Patients nolonger need to come in approximately 2 weeks before theprocedure for a laser peripheraliridotomy, meaning there is no morewaiting forexcellent results. Patient feedback isexcellent because the procedure is quick, and postsurgicalcomfort is high.
I was the first surgeon in Colorado to implant EVO. I truly believe in EVO because of the lens material and extensive data.1,2 I like that it is now a single procedure because there is no longer the need to create a hole in the iris to facilitate aqueous flow. Explantation is extremely rare, but patients like knowing that the lens is removable by a doctor if needed. Sharing the simplicity of the surgical approach with them has led to higher adoption rates in our practice and to more word-of-mouth referrals.
EVO is a great choice for vision correction for a wide range of patients, including those with moderate to high myopia (-3.00 to -20.00 D), thin corneas, or concerns about dry eye syndrome. Most of the patients I see for consultations were referred by one of our practice’s refractive surgery optometry specialists. By the time they are seen by me, they have general knowledge of the EVO procedure and other refractive surgery techniques. They know surgery, in my hands, takes about 10 minutes per eye and is painless.They also know that postoperative recovery is rapid and patients recover quickly postsurgery.3,4 During the preoperative examination, I then use very high–frequency ultrasound biomicroscopy to measure the eye accurately so that I know exactly what size EVO is appropriate for the patient. (Editor’s note: For more on sizing, see “Mastering the Preoperative Exam”) There is no guesswork.
It’s also important to let patients know what to expect after surgery. I tell them that they might notice a very short-lasting circle of light centrally when their pupils are dilated but that it will typically clear within the first night to 1 week postsurgery.
The opening in the middle of EVO is a game-changer for many reasons. In addition to eliminating the need for a preoperative peripheral iridotomy, which removes the burden placed on patients to report for a supplementary procedure a couple weeks before surgery, it also simplifies the surgical procedure. Here I share three intraoperative pearls and one postoperative pearl.
EVO surgery is straightforward, but incorporating these simple yet effective pearls can help enhance your technique and support a positive patient experience.
1. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
2. Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. 2018;12:2427-2438.
3. Kohnen T. Phakic intraocular lenses: Where are we now? J Cataract Refract Surg. 2018;44(2):121-123.
4. Wei R, Li M, Zhang H, Aruma A, Miao H, Wang X, et al. Comparison of objective and subjective visual quality early after implantable collamer lens V4c (ICL V4c) and small incision lenticule extraction (SMILE) for high myopia correction. Acta Ophthalmol. 2020;98(8):e943-e950.
With proper patient selection, outstanding safety and effectiveness is easily achievable.
The introduction of the EVO ICL lens (EVO) ushered in a new era for the ICL procedure. Now, it serves as a firstline option for patients with myopia and myopic astigmatism. Evidence has even shown the procedure to be an effective treatment for as low as -3.00 D of myopia.1 This article reviews proper patient selection and provides insight into what outcomes can be expected after EVO surgery.
Patient selection. In my practice, we position EVO as a treatment offering in place of surface ablation procedures, although we still preform surface ablation where indicated. In the past, we might have offered the procedure only for those who were not good candidates for LASIK, such as those with troublesome corneas or high myopia (>-6.00 D). Now, however, we recommend EVO for a wider range of patients such as those with a stable refractive history and moderate myopia because the implant is removable by a doctor, setting the patient up for success in the future as the needs of their eyes may change. EVO is indicated for use in patients between 21 and 45 years of age with myopia or myopic astigmatism with spherical equivalent ranging from -3.00 to -20.00 D and cylinder from 1.00 to 4.00 D at the spectacle plane, and the internal anterior chamber depth (ACD) is at least 3.00 mm. EVO should not be used in patients with a true ACD of less than3.00 mm, an anterior chamber angle less than grade III, who are pregnant or nursing, are less than 21 years of age, who have moderate to severe glaucoma, or who do not meet the minimum endothelial cell density (ECD) in the directions for use.
EVO streamlines and enhances the patient experience, and therefore many patients become interested in the technology. We also prefer EVO for those with troublesome corneas and those at risk for keratoconus based on topography or epithelial mapping.
Introducing the procedure. Our email refractive consultation appointment reminders include a brief description of the services we offer with a hyperlink to our website. We encourage patients to review the EVO information on our website, most of which was provided by STAAR. The company provides excellent resources on the benefits and risks of surgery, including compelling testimonials from influencers such as Joe Jonas, of the Jonas Brothers band (click here).
Having EVO available in the United States is a game changer. It has made the conversations we have with our patients and our consultative process much simpler. Part of our advanced vision analysis is determining what’s the best fit for the patient in front of us. In the past when we talked about the multiple vision correction procedures that we offer, the discussion about ICL surgery was a little cumbersome because we had to explain the necessity for a preoperative peripheral iridotomy. Now with EVO, however, we explain that it takes about the same amount of time as LASIK but has numerous benefits unique to EVO, which is why this has become one of the most rapidly growing procedures that we offer. We tell them that it is removable by a doctor, allowing us to create vision for a lifetime and setting them up beautifully for the future. We also tell them several studies have demonstrated that postoperative vision is as good as or better than LASIK, which provides outstanding results.2 For all these reasons, our conversion rate has increased significantly since EVO became available.
I prefer to approach EVO surgery as a same-day bilateral procedure, which we currently perform in an ambulatory surgery center. I don’t check the postoperative vault in the first eye before operating on the second eye because the vault at that time can appear to be greater than it actually is due to the timing of the assessment. The second eye is treated as an entirely new procedure with a separate sterile setup and medications and instrumentation from different manufactured lots to reduce the risk of endophthalmitis, consistent with same-day bilateral IOL surgery protocols.
On the day of surgery (between 1 and 6 hours after surgery) and at days 1 and 7, my practice checks visual acuity and IOP, and we assess the vault and centration of the lens. Postoperatively, the vault of EVO should be between 50% and 150% of the central corneal thickness (ie, 250–900 µm). If the vault falls outside this range, exchange or removal may be required only if the patient is experiencing visual symptoms (Figure 1).

Figure 1. Normal (A), shallow (B), and high (C) vault after EVO surgery.
EVO can help patients achieve freedom from spectacles and glasses. Studies have shown that EVO achieves a high level of postoperative visual acuity, refractive predictability, and stability.3 In the published literature, 90.8% of 1,905 eyes achieved an accuracy within ±0.50 D, and 98.7% were within ±1.00 D up to 5 years after surgery. The uncorrected distance visual acuity was -0.02 logMAR. In the US FDA clinical trial of 619 eyes at 6-month follow-up,1 90.5% and 98.9%, respectively, were within ±0.50 and ±1.00 D of intended correction, and the efficacy index was 1.06. The efficacy index was defined as postoperative UCVA/preoperative CDVA. Regarding CDVA, most eyes (98.5%) were the same or better at 6 months postoperative, and about half (52.3%) gained one or more lines.3
EVO provides excellent visual stability. The US FDA clinical trial also showed excellent refractive and IOP stability at months 1, 3, and 6 postoperative (Figure 2). EVO also had high predictability across a large diopter range (Figure 3).
_1683900708.jpeg)
Figure 2. Refractive (A) and IOP (B) stability at 1, 3, and 6 months after EVO surgery. Figure 3. EVO has high predictability across a large diopter range.
_1683900724.jpeg)
Figure 3. EVO has high predictability across a large diopter range.
Patients typically have excellent night vision with EVO. Studies have shown that there is significant improvement in mesopic contrast sensitivity with and without glare after EVO surgery4 with low induction of coma- and spherical-like and total higher-order aberrations.5 The rare potential for glare or halos is, however, always discussed with patients preoperatively.
EVO surgery is safe. The US FDA clinical trial confirmed that EVO has a reduced rate of anterior subcapsular cataract and pupillary block relative to earlier ICL models.1,3 Of course, all risks, benefits, and alternatives are always discussed with patients and documented.
EVO provides a quick visual recovery. Patients can expect quick visual recovery and may return to their daily activities the day after surgery. My patients are prescribed a mild steroid and antibiotic three or four times a day for 1 week.
Collectively, these outcomes point to a great potential for patients to experience these outcomes in the real-world setting.
Properly selecting patients, setting expectations, customizing the procedure, and using a meticulous surgical technique typically leads to an excellent outcome with EVO. Patients can expect the potential to achieve freedom from spectacles and glasses, stable effects, and excellent night vision.
1. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.
2. Sanders DR, Vukich JA. Comparison of implantable collamer lens (ICL) and laser-assisted in situ keratomileusis (LASIK) for low myopia. Cornea. 2003;22(4):324-31.
3. Packer M. The Implantable Collamer Lens with a central port: review of the literature. Clin Ophthalmol. 2018;12:2427-2438.
4. Martínez-Plaza E, López-Miguel A, López-de la Rosa A, et al. Effect of the EVO+ Visian phakic implantable collamer lens on visual performance and quality of vision and life. Am J Ophthalmol. 2021;226:117-125.
5. Igarashi A. Posterior chamber phakic IOLs vs. LASIK: Benefits and complications. Expert Review of Ophthalmology. 2019;14(1):43-52.
Expand your candidates, position EVO as a premium procedure, and build momentum in your community.
EVO was approved by the US FDA in March 2022. In just a little more than 1 year, the availability of this lens has had a significant impact on our business model and the way that we position the procedure to patients—as a premium option. This shift happened years ago in other countries, where EVO has been available for more than 10 years. But for those of us practicing in the United States, we can now truly offer ICL surgery for a wider range of patients. Growing your practice with ICL surgery has therefore gotten easier because surgery is streamlined, and postoperative results are proven to be safe and effective (see “What You Can Expect With Patient Outcomes”).1
IQ Laser Vision has 14 locations, six of which are equipped for surgery. We offer both laser and lens-based solutions for refractive correction because we believe that offering a multitude of procedures is the best approach to ensure patient satisfaction and increase word-of-mouth referrals. Once you know a certain procedure is best for your patient, it becomes easy to talk about with them. Comfort in recommending EVO therefore starts with a fundamental belief that the procedure is in the best interest of your patients.
The optometrists in our practice are really the gatekeepers to our patients. They meet with patients first and assess if they are a good candidate for refractive surgery in general and laser or lens-based surgery specifically. We do not work heavily with comanaging optometrists, but we have seen an increase in referrals after EVO was approved for use in the United States.
Since introducing EVO in our practice, I have increased confidence in the ICL technology for several reasons.
As I became more comfortable with the results, I started expanding my EVO candidates and usage and suggesting EVO for appropriate patients who are in the lower diopter range of myopia. I now find that eligibility for EVO extends to patients with lower amounts of myopia, those with a calculated residual stromal bed thickness of less than 280 µm, and those who may be at risk for keratoconus.
Your approach to positioning EVO will depend on your practice. For a practice like mine, which is focused on refractive surgery, the key is to portray confidence in the procedure. I first started offering the Visian ICL version 4 to patients with troublesome corneas or high myopia (>-10.00 D). When EVO was approved this past year, I began offering EVO for patients with a normal cornea and greater than -7.00 D of myopia. As more patients at our practice elected to have EVO, their friends, family, and coworkers began asking for EVO. Based on their eye condition, occupation, and visual goals, we are offering EVO to patients with as low as -3.00 D of myopia. Results of the US FDA clinical trial confirm that EVO is accurate, predictable, and stable for the correction of moderate myopia and myopic astigmatism.1
Happy patients present a great opportunity to share EVO results on social media. I treated a patient who had -20.00 D of myopia and 2.00 D of astigmatism. Right off the table after EVO surgery, she was crying because she could see clearly. Her mom was crying, too. We captured the moment and posted it to social media (with the patient’s permission). It was a powerful testimonial for the procedure and for our practice.
An even more powerful testimonial is for patients to share their experience on their own social media accounts. Everybody has a unique sphere of influence, and we have found this is an extremely helpful way to grow our business.
STAAR Surgical has done an excellent job building momentum behind EVO. Recently, three celebrities—Joe Jonas, of the Jonas Brothers band, Max Strus, who plays for the NBA’s Miami Heat, and actress Peyton List—have undergone the EVO procedure. Some patients now come in asking for EVO because they saw the campaign with Joe Jonas. It’s a very effective way to help raise awareness of the procedure among the general public.
Another helpful way we build momentum in the community is to educate our colleagues, specifically the optometry community. When optometrists are exposed to the procedure and understand the benefits and potential outcomes, they are more prepared to talk to patients about what the procedure can do for them. Over time, that builds awareness of the procedure.
Lastly, we have found it important to share successes with our staff, so they know how great the procedure is. It helps them be more authentic and enthusiastic when they talk to patients about EVO. Our counselors love to be involved when we do EVO, especially for patients with higher prescriptions or have been told they aren’t candidates for laser refractive surgery because they are so ecstatic after surgery.
One of the strongest practice builders is word-of-mouth referrals. Once you start offering EVO, more patients will be talking about it in the community. If they’ve had a great experience with the technology and with your center, they will refer their family and friends. This can have a snowball effect over time.
The single most important thing we’ve done is to get the word out in our community via social media and our website. We now have people coming in asking for EVO whereas in the past they would be asking for LASIK. We also have more patients who were told at another center that they were a good candidate for EVO coming in for a second opinion. In our experience, we confirm that EVO is the best choice for them, and they’ve had surgery at our center. Maybe they didn’t have surgery with the first doctor because it might have been the first time they’d heard about EVO. As more and more surgeons offer the procedure, patients will feel more comfortable with it as a premium refractive solution.
1. Packer M. The EVO ICL for moderate myopia: results from the US FDA clinical trial. Clin Ophthalmol. 2022;16:3981-3991.






